Answer on letter to professor E.I.Nazarov (from Velio Bocci)
Only a few days ago a colleague sent us your letter and, in order to eliminate doubts worrying several ozonetherapists, we are glad to answer the issues raised in your letter. This is now more important than ever because, after two decades of intensive work spent on clarifying the mechanisms of action of ozone in Biology and Medicine, there are now some methodological approaches invented for minimizing work that are going to jeopardize the future and acceptance of ozonetherapy within the realm of orthodox medicine. We are still struggling to prove the validity of this approach with the Food and Drug Administration (USA), that is the fundamental first step that possibly will allow the acceptance by National Health Authorities in many countries. If the Russian’s proposal of simplified and quick methods will take roots, ozonetherapy, not only will be never accepted but it will degenerate in a practice only useful for quacks , who already are too abundant.
From the outset, we want to declare to be only research scientists without any interest in whatever commercial relationship with ozonetherapy.
Topic: The need of using ozone-resistant materials to avoid toxicity.
Only well- proven ozone-resistant materials must be used to avoid toxic effects in patients.
Contrary to your statement, there is plenty of evidence published in the best international journals that various plastic microparticles, phthalates and/or other additives are released into blood components during blood storage in plastic (PVC) autotransfusion bags even during short exposure, without the presence of oxygen-ozone (O2-O3). While a minimal contamination has been tolerated, no other substance, absolutely no ozone, should be insufflated into the bag. It is necessary to remember that up to 1990 the ozonation was carried out in neutral glass bottles that are ozone resistant.
Unfortunately, later on O3-autohemotherapy (O3-AHT) has never undergone the necessary standardization so that several variants of the original procedure have been used generating an enormous confusion.
A critical examination of the various methodologies used in the last decade for carrying out O3-AHT in Italy and Germany has pointed out serious pitfalls that are potentially risky for the patient. In Italy another worrisome problem has been the widespread use of plastic (PVC) autotransfusion bags that, while suitable for storing blood, release various plastic microparticles and phthalates into the blood even without a short exposure to O2-O3 (Valeri et al., 1973; Thomas et al., 1978; Callahan et al., 1982; Estep et al., 1984; Labow et al., 1986; Quinn et al., 1986; Whysner et al., 1996; Latini, 2000; Stahlhut et al., 2007; Swan, 2008; Meeker et al., 2009; Jung et al., 2010). As it has been noted in patients undergoing dialysis, the mutagenic and toxic activity of these compounds is a matter of grave concern (Lawrence, 1978; Divincenzo et al., 1985). Particularly in the last decade there is mounting evidence that DEHP, by mimicking human hormones, may disrupt the endocrine system leading to developmental problems or behave as a mutagenic substance (Lyche et al. 2009). In January 2006, the European Union placed a ban on six types of phthalate softeners, including DEHP used in toys (Directive 2005/84/EC).
All of the following data (see Appendix 1) were published in Bocci’s book: Oxygen-Ozone therapy.
A critical evaluation, Kluwer Academic Publishers. Dordrecht, The Netherlands. 2002. Chapter 39, pp: 375-380.
We have tested several samples of plastic bags largely used in Italy for storing blood and inflow-outflow tubing in polyvinyl chloride-di(2-ethylhexyl)phthalate (PVC-DEHP). All of these bags are authorized by the Ministry of Health to store blood but not to be insufflated with O2-O3. Bags are made of PVC for a maximum content of 55% while for achieving a good elasticity additional materials amount to about 45%. With small differences the composition is the following:
a) about 40% of DEHP
b) about 1% of Zinc 2 ethyl ethylhexanoate
c) about 1% Calcium or Zinc stearate
d) about 1% N,N’-diacyl ethylenediamine
e) 5 — 10% of epoxidized soybean oil or similar.
While all bags are sterile and suitable for storing blood, they are NOT chemically inert when a strong oxidant mixture (about 250 mL) composed of about 96% O2 and 4% O3 is insufflated into the bag. Particularly DEHP and butyl-glycobutyl phthalate (BGBP) are immediately released and bound extensively to plasma lipids. The plasma is likely to yield a higher content of DEHP than physiological saline. In line with the criteria expressed by the European Pharmacopea (1997), in 1999, we carried out an investigation by using sterile physiological saline that is considered the optimal «medical device» for evaluating release and size of plastic particles (2, 5, 10, 20 and 25 m size), phthalates and other compounds. It is obvious that evaluation of contaminants could not be performed in blood. Samples were numbered and all the following tests have been carried out in a blind fashion. The code was open after the final results were available.
In conclusion it is hard to believe that you are not aware of phthalate or other additives toxicity that can harm patients receiving blood or even worse saline treated with O2-O3 in medical PVC-bags normally used only for blood storage. Thus, while hoping that this letter may be helpful, my best advice is to abolish altogether the use of plastic bags and adopt glass bottles.
You have mentioned some 1137 reports of complications some of which are most likely have been caused by plastic particles and solubilized materials infused with blood in sensitive patients.
Moreover the fate of plastic particles infused with blood taken up by phagocytosis remains a serious problem with possible late carcinogenic consequences. From 2003 up to 2007, after having supervised thousands of ozonated autohemotherapy, by both using a careful O3 dosing upgrading and the only necessary sodium citrate, no side effects have been noted. On the other hand before 1999, by unfortunately using plastic bags, especially in women, we noticed some similar side effects.
We are finally glad to read that you have now mastered the production of bags of 100% st polypropylene that you have presented at the recent Istabul Congress (1st International th th Ozonetherapy Congress, 4th-6th December 2009, Istanbul — Turkey). Thus you have come to admit the use of polypropylene container as ozone-resistant that can be safely sold. Needless to say why not to use the usual safe glass bottles?
Topic: It has now become fashionable to use the IV infusion of ozonated saline
As a physician, having practised for years in a charity clinic, I vividly remember how busy an expert dialysis technician and myself were in performing no more than a dozen O3-AHTs in a afternoon. Thus, I can well understand that in a large clinic where daily there are a hundred patients to be treated, you cannot entertain the hope to perform the classical O3-AHT and therefore one has to compromise with an uncertain and semiquantitative procedure like the IV infusion of ozonated saline or, as in the case of Cubans, to apply the rectal O3 insufflation to all patients, which, for several reasons, is an even more unreliable approach.
Almost needless to say that the classical O3-AHT, owing to the precise volume of blood, the precise volume of O3 of which one knows the exact concentration, hence the real dose, makes it an unsurpassed method. In this case the O3 instantly reacts with several blood substrates in a practically quantitative fashion. During the 5 minute mixing, we know all the biochemical reactions going on to activate blood cells so that, by the time of the reinfusion, O3 has disappeared. The beauty of the system is that, by using O3 within the well-determined therapeutic window, not only toxicity is avoided but one can control every step and fashion the ozonation process on the patient’s disease.
Since 1994, I was interested in finding a blood substitute and eventually I also landed in trying ozonating saline. As you know, it was demonstrated that ozonation of medical physiological saline (0.9% NaCl) with various O3 concentrations (50-70-100 mg/mL) induced at the same time formationof hydrogen peroxide and chemiluminescent effects indicating the generation of free radicals (Bocci et al., 1998). The production of H2O2 was progressive and by using an O3 concentration of 100 mg/mL reached the value of about 20 mM after 60 min of O3 insufflation. Without further bubbling, the infusion of 250 mL of this solution in healthy volunteers caused considerable pain along the venous path of the infused arm after about 24 hours. This indicated that the solution has irritated the endothelium with the risk of a phlebitis and we were concerned that, besides H2O2, a transitory formation of HOCl or perchlorate may be the noxious agent. Although chloride could be oxidized by O3 to perchlorate (Truong et al., 2004; Rao et al., 2010), the saline solution containing traces of 2+Fe allows to the Fenton’s reactions with formation of oxydryl ralicals Hypochlorous acid constitutes an inflammatory agent of the endothelium during an infusion, even at a trace concentration. Moreover, it may activate platelets and induce a microcoagulation. Although it is well known that ClO is physiologically produced by phagocytic cells and it is an efficacious bactericidal compound, it remains either confined in phagosomes or released in plasma near endothelial cells (Goldmann et al., 2009). However, ClO is one of the most noxious reactive oxygen species (ROS) during a chronic inflammation. It is unfortunate that the practice of using ozonated saline has become common in Russia and is widely used because it is inexpensive and less time-consuming than major AHT and simultaneously applicable to many patients. As it could be foreseen, physicians have started to use it also in Italy, Spain, Greece and Turkey. Ikonomidis et al. (2005) in Greece, have reported that they maintain the saline solution under a constant flow of O3 during transfusion but they warned that the maximum amount of O3 daily administered is usually 4-5 mg and should never exceed 8-10 mg. In their publication they also stated if we exceed these rates, the over coagulation syndrome starts and they strongly recommended to perform coagulation tests before starting therapy. These precautions reinforce our preliminary objection to this approach. Moreover, Foksinski et al. (1999) have measured 8-oxodeoxyguanosine, a typical oxidative DNA damage in lymphocytes of atherosclerotic patients after the IV infusion of ozonated saline, that is a worrisome result never detected after O3-AHT.
Fortunately to the best of our knowledge, Russian physicians ozonize the saline with very low O3 concentrations (2-3 mg/mL) and this precaution certainly reduces toxicity but it leaves open the aspect of therapeutic efficacy.
During the last couple of years I had been lucky to work together on this topic with two researchers of the Department of Pharmaceutical and Applied Chemistry at the University of Siena. We have ascertained that the procedure of ozonation of absolutely pure water is a far simpler procedure because this is the only case when the unstable O3 obeys Henry’s law. However if the water contains NaCl, the extremely high reactivity of O3 induces a complex series of reactions with the possible progressive formation of H2O2, unstable OCl , NaClO4, OH, O2 and some unstable O3. Razumovski, Ershov et al (2008); Bocci et al, (2009) have evaluated the complexity of O3 reactions and rapidity of its decomposition. Here we enclose our diagram.

Figure 1. The diagram shows the rapid increase and decrease of O3 bubbled at 70 mg/mL concentration (gas inflow 1.5 L/min) in either ultrapure water (400 mL) or physiological saline (400 mL). Ozone bubbling was stopped after 25 min and absorbance was measured every 2 min at 260 nm. At O3 concentration of 10 mg/mL the curves are very similar, but absorbance is considerably lower than shown in the diagram. (Unpublished data).
It is therefore necessary to enumerate and discuss the problems occurring during the preparation of ozonated saline:
1) For human use it would be unwise to use O3 concentration over 4 mg/mL (4 mg/L). Moreover it is essential to establish the volume per minute of the gas mixture O2-O3. The problem is that different ozone generators have variable gas output: if it is 1 L per minute, the O3 delivered to 200 mL of saline would be 4 mg/L but, if the output per minute is equivalent to 3 litres of gas, then the actual dose of O3 delivered will be 12 mg/L! As a consequence one must properly instruct the ozonetherapist in relation to the owned ozone generator as otherwise one risk to poison the patient.
2) The period of ozonation time also ought to be well defined in relation to the volume of saline because in the case of saline solution an ozonation time of 20 min appears enough to reach a plateau. Obviously a shorter or longer ozonation period will differently modifies the concentration of hydrogen peroxide, O3 and other radicals.
3) Another aspect to be clearly defined if gas bubbling will continue or not during the IV infusion period. This is because, as soon as the gas bubbling is stopped, the concentration of H2O2 remains fairly stable but the O3 concentration will halve during the next 30 min and this affects the therapeutic result. As a trivial example, I doubt that in a large clinic all the saline infusions are all under a continuous O3 bubbling and it is likely that saline bottles will be ozonated and then distributed implying a more or less long delay before the infusion. After one hour delay, O3 is not longer present.
4) As a preliminary conclusion, one must ponder on the validity of using the infusion of ozonated saline. It is certainly less dangerous than the direct IV infusion of the gas mixture that some quacks, without a medical qualification, still dare to perform with the serious risk of causing an oxygen embolism. However it does not represent a good improvement because the variable presence of H2O2, O3, etc does not insure neither a good reproducibility, nor a consistent therapeutic effect. Moreover the blood flow in the cubital vein varies considerably in different patients and in women and this implies that a fairly constant infusion of ozonated saline versus a variable blood flow and content of antioxidants implies an uncertain blood/H2O2- O3 relationship with possibly a too low or too high bio-oxidation. By comparison, a fundamental pillar of the classical O3-AHT is that we can maintain precisely the blood/ O3 ratio within the known therapeutic range.
5) I regret to say that this approach contains too many uncertain parameters and, in any case, it needs to be carefully standardized to avoid risking to perform a placebo infusion or an excessive and risky treatment. Nonetheless if, on the basis of the critical need to treat too many patient, it is allowed by Russian Health Authorities it will be never accepted by neither the FDA, USA or but the EC Authorities.
6) Owing to the fact that H2O2 is one of the most important ROS generated by O3, since 2005 (Bocci et al. 1998), in women with very difficult venous access, by using a G27 needle, we have intravenously infused the solution of pure H2O2 in glucose(5 %) or saline solutions at the concentrations ranging from 0.03-0.06 % (8-16mM). The bio-oxidative therapy with H2O2 was first described by Dr. I.N. Love in 1888 (Love, 1888) and then promoted by Dr. C.H. Farr in 1993 (Farr, 1993). We showed a modest but consistent activity in women with age-related macular degeneration. In contrast to ozonated saline, this compromise, very simple to prepare, does not contain other dangerous ROS and one does not need an ozone generator. Obviously, the glucose solution should not be used in diabetic patients.
Finally, I am also very interested in treating chronic heart disease (CHD) and I would like to call your attention to the disastrous result published in the Lancet (Torre-Amione et al., 2008), by using a bad copy of minor AHT after an extremely high oxidation and heat stress on 10 mL of blood. This is a dreadful example of an irrational ozonation procedure that has severely compromised the future of ozonetherapy. The study by Dr A.V. Artiomenko (Odessa, 2004) performed with ozonated saline seems to have given a significant (statistic is missing!) improvement of 63 CHD’s patients. However, what is missing in this study is a direct comparison with a similar group of patients properly treated with O3-AHT. As it is, results not published in an international peer reviewed journals are lost for the scientific community.
Summary We would like to thank you for your letter and for compelling us to express our objective judgements. Our aim is to try to demonstrate the validity and reliability of ozonetherapy and all our efforts should be directed to allow the acceptance of ozonetherapy as an effective approach within orthodox medicine. The Western world is either against or it has prejudice towards this approach and, in spite on lack of sponsors and funds, we must strive hard to succeed.
V. Bocci, MD, Emeritus Professor of Physiology, Department of Physiology,
Prof. V. Travagli, and Dr. I. Zanardi, PhD, Department of Pharmaceutical and Applied Chemistry at the University of Siena, Italy
16/04/2010
Appendix 1
1. MATERIALS AND METHODS
Particles were measured by an automatic counter (Royco) by Dr. G. Gavioli and collaborators at Braun Carex, Mirandola (Modena, Italy) while several chemical compounds among which phthalates were detected by HPLC by a specialized Institute (Istituto di Ricerche Agroindustria, Director: Dr. G.C. Angeli, Modena, Italy).
The proliferation index (PI) of blood mononuclear cells (BMC) has been assessed after isolation of BMC from human blood of normal donors. PBMC were isolated by Ficoll-Hypaque (Sigma Chemical Co., St. Louis, MO) gradient centrifugation, washed twice in RPMI-1640 medium supplemented with 20 mM HEPES buffer, spun down at low speed to remove platelets, and resuspended in RPMI-1640 medium supplemented with 2 mM HEPES, 10% heat-inactivated fetal calf serum (FCS), 2 mM L-glutamine, 100 U/mL penicillin and 100 mg/mL streptomycin (all from Life Technologies, Gaithersburg, MD) at the final concentration of 1 x 10 viable cells/mL. Cell viability was assayed by the trypan blue exclusion technique and light microscope observation. Aliquots (0.1 mL) of BMC suspension were added per well in triplicate wells to 96-well flat bottomed tissue culture plates (Costar, Cambridge, MA). BMC were cultured without stimulation or stimulated with PHA at a final concentration of 5 mg/mL (Sigma Chemical Co.). After 12 hours incubation, either control saline, or ozonized saline in a glass syringe, or in blood bags was added to the culture medium in a 1:4 proportion. Thereafter incubation continued for 40 and 64 hours. Cell proliferation was evaluated by a colorimetric immunoassay (Boehringer Mannheim, Mannheim, Germany) based on BrdU incorporation. Briefly, after either 40 and 64 hours of incubation at 37 with 5% CO2 in air and 100 % humidity, the cells were labelled with BrdU for 6 hr (10 IU/well). The cells were then fixed, anti-BrdU-POD antibody added and the immune complexes detected by the subsequent substrate reaction. The proliferative index (PI) was obtained, calculating the ratio between PHA-stimulated cells and unstimulated ones, after subtraction of the corresponding blanks. It is emphasized that all tests were carried out with the same procedure and timing used during a conventional autohaemotherapy.
All tests were performed in double blind fashion by two external firms specialized in the pertinent assays. PI and all other analyses were assessed in the Institute of General Physiology, University of Siena. Results were expressed as mean+/-SD.
2. RESULTS AND DISCUSSION
These can be summarized as follows:
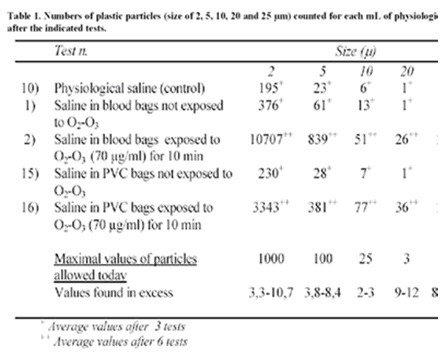
Table 1 reports the number of plastic particles ranging in size among 2, 5, 10, 20 and 25 mm in either the control saline (test no. 10), or in saline withdrawn from blood bags with no exposure to O2-O3 (test no. 1) or in saline as before but exposed to O2-O3 (70 mg/mL per mL saline, ratio 1:1) for 10 min (test no. 2), or in saline from other PVC bags, control (test no. 15) or in saline exposed to O2-O3 for 10 min (test no. 16). It appears very clear that the number of plastic particles released from different PVC blood bags far exceed the number of control samples. According to the European Pharmacopea, values of particles released after ozonation exceed the maximal tolerated value of 3.3-10.7 fold. All the saline samples collected from the plastic bags after ozonation showed by HPLC examination, several compounds as phthalates, caprolactamate and linear chain hydrocarbons not readily identifiable.
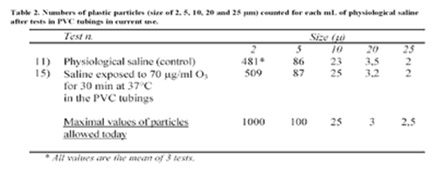
Interestingly, the same examination of tubing in PVC-DEHP normally used for collecting blood and insufflating O2-O3 do not show an abnormal release of plastic particles (Table 2) even though the O3 exposure was prolonged for 30 min. This is not surprising because tubings have far less additives than bags. Thus as the time of contact with O2-O3 is very transient, these tubings could still be used although we have preferred to substitute them with a new brand made up of more resistant material (PVC additioned with tris(2-ethylhexyl) trimellitate, TEHT, C33H54O6) known as Staflex TOTM. Material released from this type of tubing is less than 100 fold than from tubing PVC-DEHP so that this new type is absolutely safe.
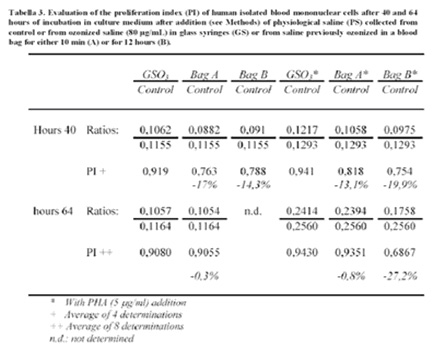
Besides the potential risk propounded by plastic particles and chemical compounds during the reinfusion of ozonated blood, we thought important to investigate whether BMC withdrawn from the bags show any modification of the PI. A series of analyses carried out after two different periods of incubation (40 and 64 hours) clearly show a consistent depression of the PI that can be as high as 27.2% (Table 3). Taking into account the small volume of ozonated saline added to the culture medium this value is possibly underestimated and therefore is worrisome. This negative effect is not directly due to O3 but rather to unknown compounds released into the saline during ozonation of the blood bags. It is obvious that we do not want the same phenomenon occurring in vivo and moreover, owing to the variety of compounds released from the plastic material, we don’t know which is (are) the compound(s) responsible for the inhibition.
For all of these reasons, the use of a new device is now strongly recommended. This is composed of a) a neutral 500 mL glass bottle (sterile and under vacuum), b) a new atoxic tubing for collecting blood and insufflating sterile-filtered O2-O3 via an antibacterial (0.2 mm), hydrophobic ozone-resistant filter and c) an appropriate tubing with filter that is used, firstly for infusing saline, and secondly for returning the ozonated blood to the donor.
It is important that the exposure of blood to O2-O3 lasts only the necessary 5 min because mixing of blood must be gentle to avoid foaming. Because blood is very viscous, it takes about 5 min to achieve a complete and homogenous equilibrium. It can be noted that the pO2 slowly reaches supraphysiological values (up to 400 mmHg) and then it remains constant. On the other hand, O3 rapidly dissolves in the water of plasma and then reacts instantaneously so that all of the O3 dose is exhausted within 5 min.
The ozonetherapists must follow this procedure for avoiding either negative effects on the patients, or being found guilty of medical malpractice.
The worrisome problem is the widespread use of plastic autotransfusion bags that, while suitable for storing blood, release various plastic compounds into the blood, especially lipids, even during a short time.
The data were sent to The Italian National Research Health Institute in Rome. The answer was that plastic bags allowed for storing blood CANNOT BE USED WITH O2-O3 IN ANY CIRCUMSTANCE. The prohibition became and remains effective since 2000: Today CE neutral glass bottles fitted with ozone-resistant plastic cork and idoneous tubings are currently used.
You also can download this article in PDF file by this link